INTRODUCTION
About 75% of bladder cancer is non-muscle invasive bladder cancer (NMIBC). Transurethral resection of bladder tumor (TURBT) combined with intravesical chemotherapy-immune drug perfusion is the standard treatment of NMIBC. Repeat transurethral resection of bladder tumor (Re-TURBT) can detect and remove residual tumors, correct tumor grading and staging errors, and may ultimately lead to changes in the treatment strategy and prognosis. Therefore, the current European Association of Urology (EAU) guidelines point out that the secondary resection must be performed only when the first resection of bladder tumor is incomplete, and the secondary resection is recommended for high-grade and/or T1 tumors that can be completely resected [
1]. However, the recurrence rate post secondary electroresection is not high, which could increase the likelihood of iatrogenic trauma and economic burden for bladder cancer patients, and, therefore, the selection of right patients is of great importance [
2]. In this study, fluorescence
in situ hybridization (FISH) was used to detect the aberration of chromosome 3
, 7
, 17 and GLPp16 on chromosome 9 in urine exfoliated cells of patients before secondary electroresection, and to explore the diagnostic value of FISH in the secondary electroresection.
PATIENTS AND METHODS
Data of cancer patients
Upon the approval of the Department Review Committee, 26 patients with bladder urothelial carcinoma treated in Tongji Hospital were subjected to FISH detection before the second resection from January 2016 to April 2022, and all of them satisfied the recommended indications for the second resection in the EAU guidelines (Some for insufficient TURBT, some for T1 tumor, some for grade G3, some for lack of muscularis propria in first-TURBT). The negative controls were selected from 100 patients with hematuria, who were diagnosed as having non-urothelial carcinoma by imaging examination and cystoscopy.
Chromosome 3, 7, 17 and GLPp16 on Chromosome 9 probes were used for FISH detection. Specifically, 200 mL of morning urine was collected before operation and sent for examination within 1 hour.
Analysis of FISH results
The FISH results was reviewed double-blindly by two professionally certified pathologists with ten years of working experience. Two red and two green signals were observed in normal nuclei on Chromosomes 3, 7, 17 and diploid at GLPp16 site on Chromosome 9. A non-diploid change in the cell different from the above-mentioned diploid was deemed abnormal (Fig.1). At least 25 tumor cells were analyzed. If four or more cells with chromosome abnormalities (increase of spot number of Chromosomes 3, 7 and 17 by one or more or > 10%) were positive for FISH, or the p16 locus deletions in the nucleus were less than 2 (or the deletion ratio was more than 15%), the diagnosis of bladder urothelial carcinoma could be established (Fig.2). The normal threshold was determined based on the results of 100 patients with hematuria due to benign urinary diseases, and the spot number of each sample was determined against the threshold. If the detection value was greater than the threshold, the diagnosis of bladder urothelial carcinoma could be made and if the value was less than the threshold, the result was taken as negative.
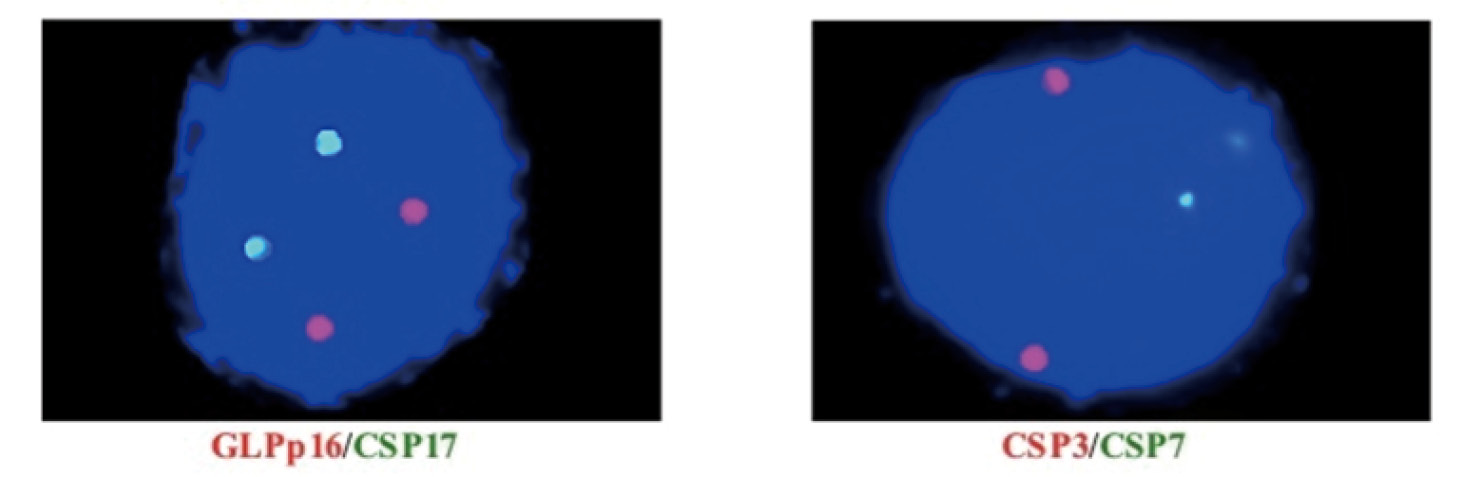
Figure 1 Normal FISH test results: After chromosome hybridization in the cell, there should be 2 green and 2 red fluorescence spots, indicating that there was no amplification of Chromosomes 3, 7 and 17, and no deletion of GLPp16 site. Red represents CSP3 and GLPp16, green is indicative of CSP7 and CSP17.
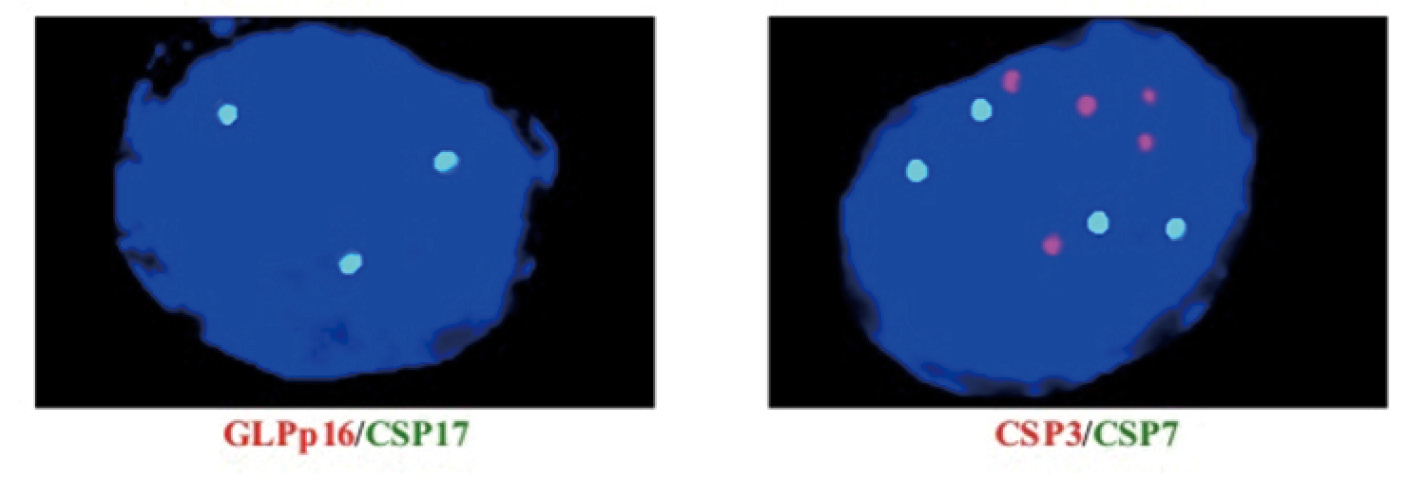
Figure 2 Abnormal urine FISH test results: After chromosome hybridization, the cells should show no two green and red fluorescence spots, namely Chromosome 3, 7, 17 amplification, GLPp16 deletion. Red indicates CSP7 and GLPp16, green spot represents CSP3 and CSP17.
Statistical Analysis
The data were analyzed by employing SPSS 26.0, and the postoperative pathological diagnosis was used as the gold standard. Counting variables were expressed as frequency, ratio, and percentage. The chi-square test was utilized to compare the classified variables. When the data were limited, Fisher’s accurate test was used to calculate the sensitivity and specificity of FISH before secondary electroresection. A P < 0.05 was considered to be statistically significant.
RESULTS
The detection rate of urinary FISH before and after secondary electroresection
All 26 patients were followed up for 2‒8 weeks after the first TURBT. Eight cases recrudesced, including 6 FISH-positive cases and 2 FISH-negative patients, and 18 cases did not develop tumor recurrence, including 1 FISH-positive cases and 17 FISH-negative ones. Overall, 85.71% of FISH-positive patients developed recurrence after secondary electroresection, and only 10.53% (2/19) of FISH-negative patients had tumor recurrence after secondary electroresection. The result indicated that the recurrence rate of bladder cancer in patients positive for FISH test before secondary electroresection was higher than in their counterparts negative for FISH (χ2 = 13.576, P < 0.01). The sensitivity, specificity and accuracy of FISH in the detection of bladder urothelial carcinoma before secondary electroresection were 75%, 94.44% and 88.46%, respectively. The results of FISH detection and pathologies of 26 patients receiving secondary electroresection are shown in Table 1.
Table 1. FISH detection and pathological results of patients undergoing secondary electroresection
|
|
|
|
|
| Recurrence |
6 |
2 |
8 |
| No recurrence |
1 |
17 |
18 |
| Total |
7 |
19 |
26 |
Chromosome aberration and gene deletion in patients positive for urine FISH test after secondary electroresection
Among the 26 patients included in the study, the proportion of increased spot number of Chromosomes 3, 7 and 17 and the deletion rate of GLPp16 gene in FISH-positive patients before the first electroresection were 83.33% (5/6), 83.33% (5/6), 50% (3/6) and 33.33% (2/6), respectively. In the FISH-positive patients, before the second electroresection, the proportion of amplification of Chromosomes 3, 7 and 17 and the deletion rate of GLPp16 gene were 100% (7/7), 100% (7/7), 85.71% (6/7) and 14.29% (1/7), respectively. No significant difference was found in the spot number of Chromosomes 3, 7 and 17 and the deletion rate of GLPp16 gene before and after electroresection. The specific results are shown in Tables 2 and 3.
Follow-up results of bladder tumor patients after secondary electroresection
Twenty-six patients were followed up for 6 months. Among the 8 recurrent patients, 6 cases were pathologically shown to be high-grade urothelial carcinoma of the bladder while the other 2 cases were focal urothelial carcinoma in situ. Two patients with high-grade urothelial carcinoma recurred and received radical resection of bladder cancer within 3 months after secondary electroresection, while the other 6 patients were treated with intravesical perfusion of chemotherapeutic drugs after secondary electroresection. During the follow-up period, no recurrence was found in 18 pathologically-negative patients after secondary electroresection.
DISCUSSION
As we know, bladder cancer is prone to recurrence. Early prediction of tumor recurrence can improve the therapeutic effect and prolong the survival time of patients [
3]. At present, the clinical follow-up of bladder cancer patients mainly uses cystoscopy and cytological analysis of exfoliated cells in urine, generally at an interval of 3‒6 months. However, cystoscopy, as an invasive examination, inevitably increases the injury and pain of patients, making it difficult for most patients to accept, and leads to unsatisfactory consequences. In recent years, urine FISH detection has been widely used as an effective means for the early diagnosis of bladder cancer. Skacel
et al. [
4] reported that the sensitivity of FISH in the diagnosis of bladder cancer was 85%, and the specificity was 97%, and FISH can also effectively predict postoperative recurrence of bladder cancer. The basic principle of FISH detection involves the use of fluorescence-labeled DNA probes to identify chromosomal aberrations associated with bladder cancer, such as the polyploidy of Chromosomes 3
, 7 and 17 and the deletion of GLPp16 gene loci on Chromosome 9. Therefore, FISH can be used to detect the aberration of Chromosome 3
, 7 and 17 and GLPp16 gene in urine exfoliated cells to diagnose bladder cancer and monitor the recurrence of bladder cancer. FISH, as a molecular detection technique, can detect changes in the number of nuclei and chromosomes during the interreplication phase of cells, and, therefore, can detect tumors in advance at the molecular level and identify tumors before histopathological changes occur. It has been extensively used, as an auxiliary tool, in the early diagnosis of bladder cancer and the recurrence monitoring. A number of follow-up studies [
5] have shown that in patients diagnosed with bladder cancer, about 60%‒70% of FISH-positive patients definitely developed tumor recurrence during the follow-up, while only about 10%‒20% of FISH-negative patients clearly suffered from tumor recurrence. These results indicated that the interpretation of FISH results is particularly important for the recurrence diagnosis of bladder cancer. Previous studies [
6] confirmed the clinical value of FISH in the monitoring of early postoperative recurrence of bladder urothelial tumors, but its application in preoperative diagnosis of secondary electroresection has not been reported in the Chinese population.
Table 2. Chromosome status of FISH-positive cases before the first electroresection
|
|
|
|
|
|
|
|
|
| 1 |
Male |
62 |
High grade urothelial carcinoma |
1 |
1 |
0 |
1 |
| 2 |
Male |
58 |
High-grade urothelial carcinoma |
1 |
1 |
0 |
0 |
| 3 |
Male |
55 |
High-grade urothelial carcinoma |
1 |
1 |
0 |
1 |
| 4 |
Male |
61 |
High-grade urothelial carcinoma |
1 |
1 |
0 |
0 |
| 5 |
Male |
75 |
Low-grade urothelial carcinoma |
0 |
0 |
1 |
0 |
| 6 |
Male |
48 |
High-grade urothelial carcinoma |
1 |
1 |
1 |
1 |
Table 3. Chromosome status of FISH-positive cases before the second electroresection
|
|
|
|
|
|
|
|
|
| 1 |
Male |
62 |
High grade urothelial carcinoma |
1 |
1 |
0 |
1 |
| 2 |
Male |
57 |
High-grade urothelial carcinoma |
1 |
1 |
1 |
1 |
| 3 |
Male |
63 |
High-grade urothelial carcinoma |
1 |
1 |
0 |
1 |
| 4 |
Male |
59 |
Urothelial carcinoma in situ |
1 |
1 |
0 |
1 |
| 5 |
Male |
55 |
The second electric cut is normal |
1 |
1 |
0 |
0 |
| 6 |
Male |
65 |
High-grade urothelial carcinoma |
1 |
1 |
0 |
1 |
| 7 |
Male |
58 |
Urothelial carcinoma in situ |
1 |
1 |
0 |
1 |
Herr
et al. [
7] found that secondary resection is an important way to reveal the true tumor load, myometrial invasion and the widespread existence of high-grade T1 tumors. Not only could it remove residual tumors and correctly identifies tumor stages, but also adjust treatment plans and improve the prognosis of patients. Therefore, secondary resection is a diagnostic, therapeutic and prognosis-improving surgery, which can better treat high-risk NMIBC. In this study, 2 patients were pathologically diagnosed as having high-grade invasive urothelial carcinoma of the bladder after secondary electroresection, and both of them underwent radical resection of bladder cancer. At present, all guidelines recommend TURBT as the main method for the treatment of NMIBC, but it still has some deficiencies when put into clinical application. The main manifestations are as follows: (1) The cancer tissue can not be completely removed by the procedure and the postoperative residual rate is high; (2) the operation and efficacy evaluation are not unified and standardized, and they are subject to biases; (3) after electroresection, the postoperative pathological diagnosis is difficult to achieve the standard [
8]. Since the aforementioned problems are inevitable, it is difficult to establish an accurate diagnosis and stage bladder cancer in clinical practice. These factors affect the ensuing treatment and prognosis of patients to a great extent, causing some patients to delay the radical cystectomy. In addition, tumor patients after TURBT often have severe lower urinary tract symptoms in a short period time due to the impact of surgical procedures and chemotherapeutic drugs. Therefore, it is urgent to work out an accurate detection method to provide guidance to the patients in the second electroresection. This study showed that the detection of urinary FISH in patients within 2‒8 weeks after TURBT is helpful for the monitoring and early evaluation of bladder urothelial carcinoma recurrence before secondary electroresection. The recurrence rate of FISH-positive patients was significantly higher than their FISH-negative counterparts, especially those who were persistently positive for FISH before secondary electroresection, and we should be highly aware of the possibility of its progression. Therefore, for these patients, in addition to secondary electroresection, further comprehensive management may be needed, such as a postoperative combination of BCG (Bacillus Calmette-Guerin), shortening the time of cystoscopy, among others. In this paper, the sensitivity of urine FISH to detect bladder urothelial carcinoma before secondary electroresection was 75%, which was slightly different from 62.2% reported by Dimashkieh
et al. [
9]. The discrepancy might be ascribed to differences in population, experienceof the surgeon and the methods of postoperative bladder perfusion. A prospective study in patients with suspected urothelial carcinoma positive for FISH but negative for cystoscopy [
10] showed that 28.9% of the patients progressed to tumor at 1-year’s follow-up, whereas in patients with suspected urothelial carcinoma negative for both FISH and cystoscopy, only 9.7% of patients developed tumor after 1-year follow-up. Regarding the application of FISH in bladder cancer surgery, studies have shown [
11] that for patients who underwent FISH examination at 6 weeks, 3 and 6 months after bladder cancer surgery, the recurrence rate of bladder cancer in patients positive for FISH was substantially increased. To sum up, patients positive for FISH after surgery are at a higher risk of recurrence. Patients positive for FISH but negative for cystoscopy should be closely followed up on long-term basis to detect recurrent tumors in time. However, for bladder cancer patients who are indicated for secondary electroresection, the recurrence rate following secondary electrotomy in patients negative for FISH is low, so cystoscopy can be performed first before deciding whether to perform secondary electrotomy, so as to reduce the pain and economic pressure of patients.
In terms of the effect of secondary resection on the prognosis of patients, Calo
et al. [
12] conducted a retrospective study involving 118 patients receiving secondary resection. Their results showed that secondary resection in patients with high-grade T1 bladder tumors completely resected failed to achieve a more favorable prognosis. This is consistent with the results of two patients in this study who were diagnosed with postoperative recurrence of high-grade invasive urothelial carcinoma of the bladder and underwent radical resection of bladder cancer. Palou
et al. [
13] also confirmed that, for patients with T1G3 (Tumor 1 Grade 3), secondary resection had no advantage in terms of recurrence rate and tumor-specific mortality compared with patients treated with BCG after TURBT, suggesting that the candidates of secondary resection should be further screened and optimized by taking prognosis improvement into consideration.
Urothelial carcinoma of the bladder is a condition that entails long-term observation and follow-up. Currently, CTC (Circulating Tumor Cell) capture, and methylation detection are developing rapidly and can identify the tumor cells in urine. Due to the substantial discrepancies in laboratory results of current studies on urinary DNA methylation for the diagnosis of bladder cancer [
14], further technological breakthroughs and larger prospective studies are needed to confirm its application in the diagnosis of bladder urothelial carcinoma. The patient population and follow-up time in this study did not suffice to fully assess the disease. Prospective, and large-sized sample studies are warranted to further confirm the application value of FISH in efficacy evaluation of the secondary electroresection of bladder tumors.
CONCLUSIONS
To sum up, for bladder cancer patients who are indicated for the secondary electroresection, urinary FISH is still an effective, convenient and rapid method to evaluate whether there is residual or recurrent tumor, which can further guide the decision about the performance of secondary electroresection. If a patient indicated for secondary electroresection is found to be negative for urinary FISH, the recurrence rate after secondary electroresection is relatively low. Therefore, cystoscopy can be performed first, and then decide whether to perform secondary electroresection.