INTRODUCTION
Bladder leiomyomas are benign mesenchymal tumors of the bladder. However, the neoplasms are very rare, with approximately 250 cases reported globally [
1]. The incidence is similar in men and women. Patients may be asymptomatic or present with lower urinary tract symptoms or hematuria. Direct cystoscopic visualization is useful in determining the location of the tumor in relation to the bladder lumen. Small tumors in accessible locations may be treated with a transurethral resection of the bladder tumor, although tumors in an unfavorable position or undifferentiated may require segmental resection or partial cystectomy [
1].
Diagnostic imaging helps in the differentiation of bladder leiomyoma from other tumors. However, the difficulty in diagnostic evaluation lies in the significant overlap between the images of leiomyoma and leiomyosarcoma as shown by Computer Tomography (CT) and Magnetic Resonance Imaging (MRI). The utility of 18F-fluorodeoxyglucose (FDG) positron emission tomography/computerized tomography (PET/CT) has not been well studied in benign bladder lesions. In this case report, we evaluated the utility of FDG-PET/CT in characterizing an undifferentiated bladder tumor and reviewed the existing literature on this topic.
CASE PRESENTATION
A 41-year-old female was referred to our clinic with a five-month history of intermittent right anteromedial thigh pain and urinary frequency and urgency. She had no major medical issues. She was a past smoker, with no occupational risk factors for urothelial malignancy.
Urine culture and cytology confirmed no infection or malignant cells. Ultrasound demonstrated a hypoechoic lesion on the right anterior bladder wall, measuring 44 × 42 × 28 mm. CT showed a soft-tissue attenuation mass protruding into the bladder lumen, exhibiting equivocal mild lesional enhancement. MRI demonstrated a heterogenous bladder tumor appearing intramural, rather than intraluminal (Fig. 1). The mass was mobile on bimanual examination and cystoscopic evaluation visualized a large mass indenting the right bladder wall (Fig. 2). A transurethral resection biopsy was considered but not performed for the concern of spreading a malignant process.
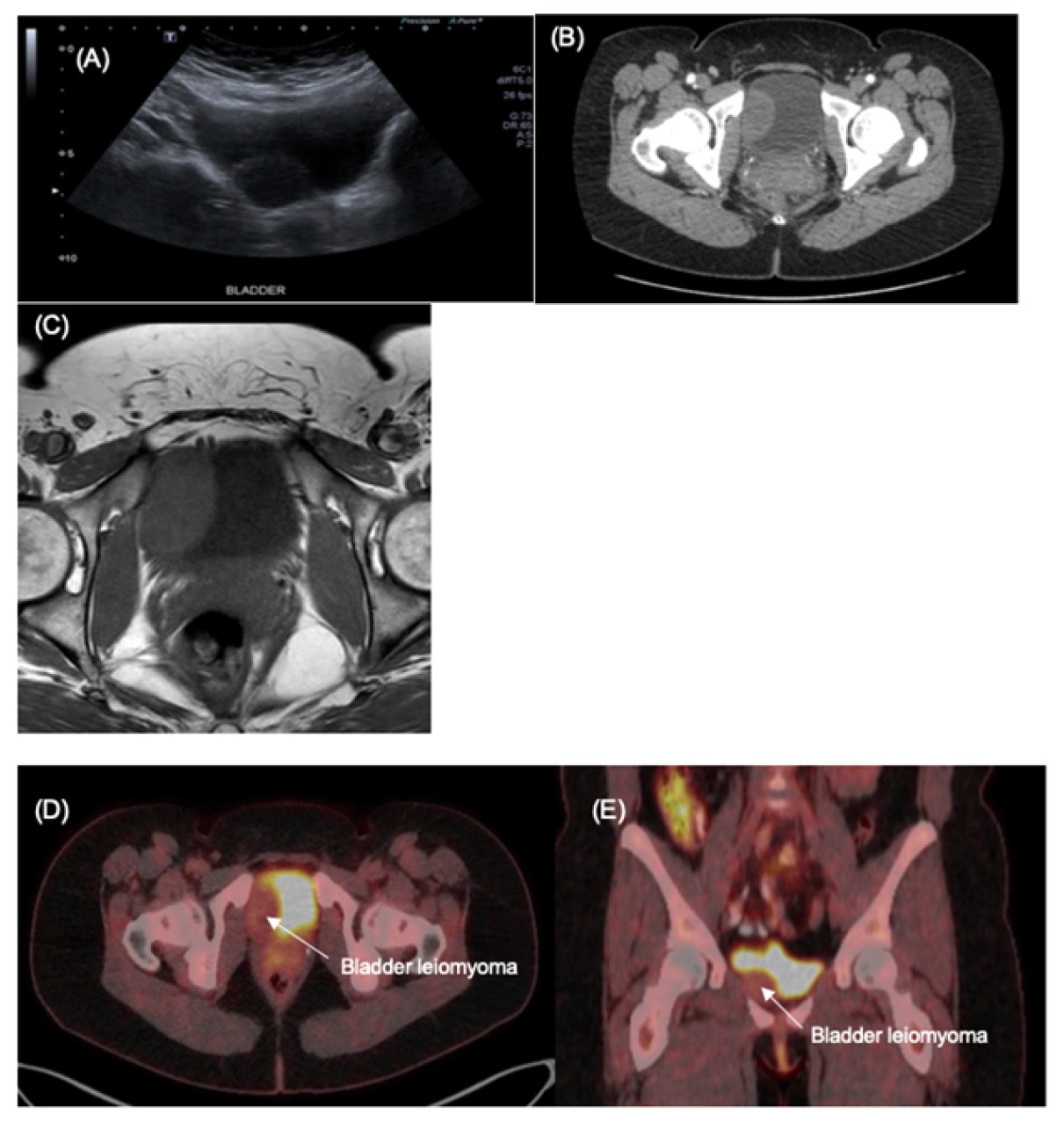
Figure 1. (A) Sonographic appearance of hypoechoic mass arising within the bladder wall; (B) Axial CT demonstrating a smooth contour soft tissue density within the inferior bladder; (C) MRI T1 weighted axial image demonstrating that the lesion had similar intensity to muscle; (D) Axial FDG-PET/CT demonstrating mild FDG uptake in bladder lesion (SUVmax 3.2); (E) Corresponding Coronal FDG-PET/CT
Her case was reviewed at our institutional multi-disciplinary meeting, given concerns that it could represent a rare sarcomatous process. A FDG-PET CT was performed and low-grade FDG uptake (metabolic activity) was displayed with no avid nodal or distant metastatic disease (Fig. 1).
A partial cystectomy was planned with the impression that this lesion was likely intramural and was not sarcomatous. Intra-operatively the mass was noted to be extramural and adjacent to the right inferolateral bladder wall (Fig. 2). The lesion was circumferentially dissected free and partial cystectomy was avoided. Her post-operative recovery was uneventful. Histopathology confirmed leiomyoma with the tissue composed of interweaving bands of bland smooth muscles with no cell atypia.
DISCUSSION
Bladder leiomyomas are rare benign mesenchymal tumors [
1]. Diagnostic imaging assists in differentiating bladder leiomyoma from other tumors. Sonographic examination typically reveals a hypoechoic mural lesion. CT characterizes the location in relation to the bladder lumen, and may demonstrate little to moderate contrast enhancement [
1]. On MRI, leiomyomas present as relatively low signal on T2 weighted images and low to intermediate signal on T1 weighted images. However, the differentiation is rendered difficult by the significant overlap between CT and MR appearance of leiomyoma and leiomyosarcoma (particularly low-grade variants) [
2].
FDG-PET/CT may be a useful modality when the malignant potential of a bladder lesion remains unclear, as it was the case in this patient. Its utility has not been well studied in benign bladder lesions. However, the literature is more robust for uterine lesions. Higher FDG tracer uptake (maximum Standardized Uptake Value [
SUVmax]) correlates with higher tumour grades in uterine leiomyosarcomas [
3]. Conversely, low SUV
max have been found to be associated with uterine leiomyomas [
4]. However, uterine leiomyomas may have variable SUV
max, with some variants having SUV
max intense enough to resemble leiomyosarcoma [
5].
A single case report described the use of FDG-PET/CT for staging in bladder leiomyosarcoma, which demonstrated an intense FDG-avid bladder lesion [
6]. In our case, PET/CT was able to distinguish between bladder leiomyoma and high-grade leiomyosarcoma based on FDG uptake intensity. However, limitations include lack of specificity in distinguishing between leiomyoma and low-grade leiomyosarcoma – both may display low SUV
max. Furthermore, there is potential for false negatives as necrotic or mucinous leiomyosarcomatous variants may demonstrate low-level FDG uptake.
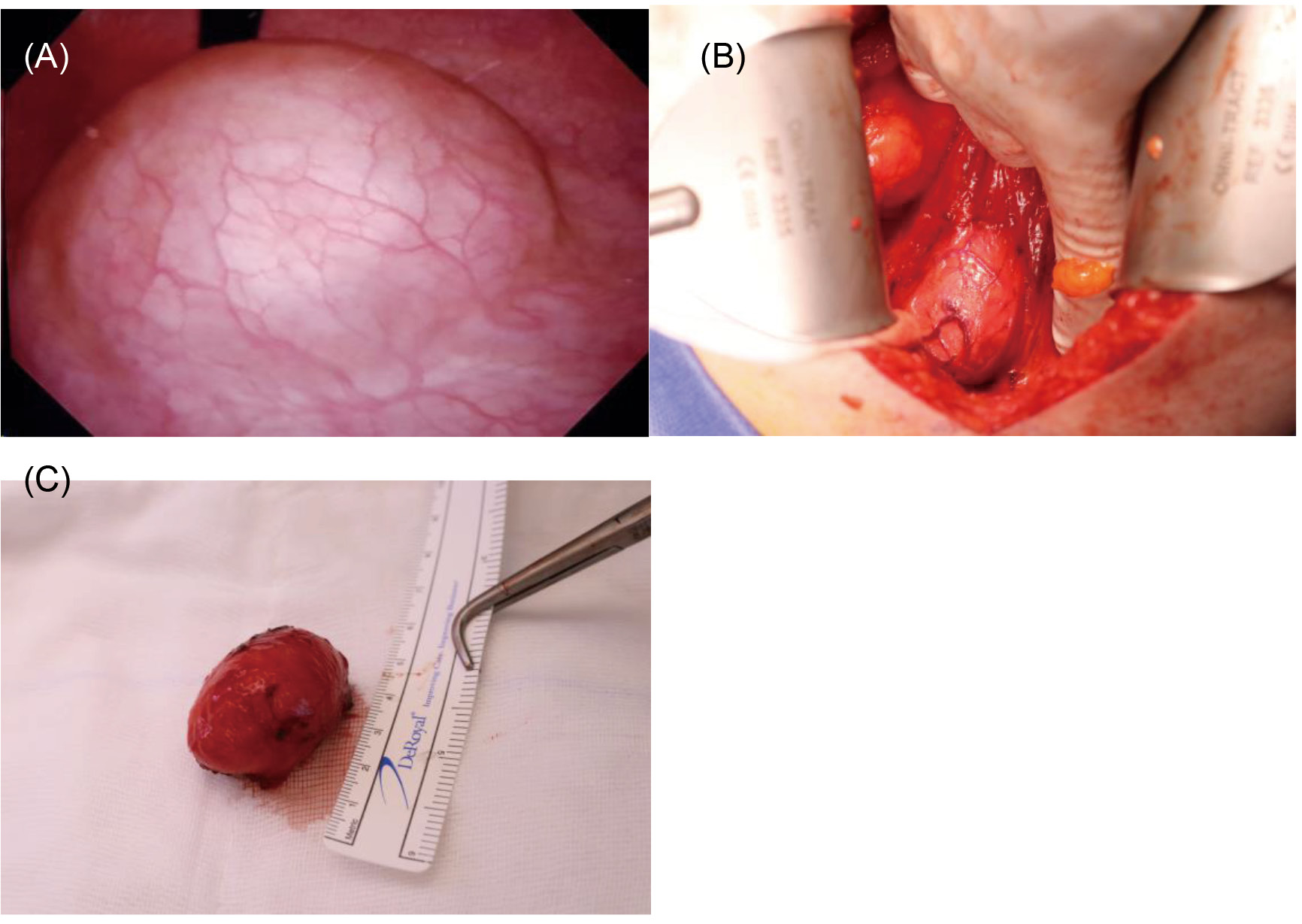
Figure 2. (A) An intraoperative photo of bladder leiomyoma on cystoscopic evaluation; (B) An intraoperative photo of bladder leiomyoma in situ, attached to bladder wall; (C) Bladder leiomyoma after excision
Review of the literature yielded one case report that described FDG-PET/CT evaluation of bladder leiomyoma [
7]. Similar to our case, the bladder leiomyoma had low FDG avidity but still raised suspicion for a low-grade cancer. Our case differed as sonographic and CT features strongly suggested a leiomyoma. However, leiomyosarcoma was considered given the small area of diffusion restriction on MR. FDG-PET/CT was influential in informing operative planning as low FDG uptake and absence of metastatic disease made leiomyosarcoma much less likely. This allowed the surgical team to avoid a radical cystectomy and plan for less aggressive surgical extirpation, such as a partial cystectomy, which is the suggested option for intramural or extravesical leiomyomas [
1]. FDG-PET/CT also provided assurance for safe conversion to tumour excision intraoperatively.
CONCLUSION
Bladder leiomyomas are very rare. Preoperative planning to confirm diagnosis is not standardized. This paper highlighted the utility of PET imaging in confirming the metabolic activity of benign bladder lesion , facilitating selection of potentially less radical treatment and bladder-conserving surgery.