INTRODUCTION
Bladder voiding efficiency (BVE) is measured according to the degree of bladder emptying and defined as the ratio between voided volume and total bladder capacity [
1]. This simple index allows to compare post-void residual volume (PVR) with the volume of urine in the bladder at initiation of voiding (V
ini = volume initial = voided volume + residual volume).
Bladder voiding efficiency is easy to calculate but not widely used. Cholhan
et al. [
2] have evaluated bladder voiding efficiency from 2 successive free uroflowmetries (FF) in pre-menopausal women during proliferative and secretory phases of the menstrual cycle. They concluded that BVE was “a clinically meaningful method” of assessing bladder emptying. In their study on Trans-Obturator Tape (TOT), Park
et al. [
3] showed a decrease of emptying efficiency in the early post-operative period. Choo
et al. have used bladder voiding efficiency to suggest that large PVR (low bladder voiding efficiency) were associated with “relatively” slight improvements in short term surgical outcomes after GreenLight HPS
TM laser photoselective vaporization of the prostate [
4].
To our knowledge, none of these studies have compared bladder voiding efficiency measurements resulting from a FF versus an intubated flow (IF) to determine the most appropriate use of this index. Therefore, the goal of our study was twofold: first compare bladder voiding efficiency findings from two separate voiding events during a urodynamic study (UDS), namely bladder voiding efficiency with FF (BVE FF) then with IF (BVE IF); and then correlate bladder voiding efficiency measurements with urinary incontinence presenting complaints (or indications for UDS referral) and with UDS findings.
Materials and Methods
This study was conducted in accordance with the Declaration of Helsinki. According to the local practice of our Ethics Committee, there was no formal Institutional Review Board approval required for retrospective studies.
UDS recordings of women who were referred for lower urinary tract dysfunction (LUTD) evaluation to our urodynamic centre over a 3-year period were reviewed. Exclusion criteria included history of neurological disease, diabetes mellitus, or stage ≥ 2 prolapse and voided volume, either from FF or IF, lower than 100 ml.
Urodynamic sessions were performed using the Dorado® unit from Laborie. Each analyzed file included FF at arrival, in private condition (sitting position), a filling cystometry and then a voiding study with an IF. Cystometry was performed with the patient in a sitting position with a 7-F triple-lumen urethral catheter perfused with saline at room temperature using a filling rate of 50 ml/min. PVR after FF were measured using the catheter introduced for the filling cystometry; after IF, PVR was also obtained through the same catheter, before re-filling for the urethral profilometry. Women who were not able to void during the study or who expelled the catheter during IF, were excluded.
All patients had dipstick urinalysis on the day of the test to confirm no ongoing urinary tract infection; if a woman had a history of urinary tract infection, urinalysis was required one week before the study and, if positive, an antibiotic treatment was prescribed.
Statistical analysis
The numerical data are described by means and standard deviation. The paired t-test was used for comparison of related samples. Analysis of variance was used to compare unrelated samples. Statistical analysis was performed using SAS, version 5.0 (SAS Institute, Inc., Cary, NC). All statistical results were considered significant at P < 0.05.
RESULTS
Over the past 3 years, one hundred and eighty eight UDS studies met study criteria for FF and IF of volumes ≥ 100 ml. Mean age was 58.3 ± 14.9 years (range, 21–90). Urinary incontinence presenting complaint included stress urinary incontinence (52), urge incontinence (65), mixed incontinence (71).
Analysis of the whole population
Overall, volume voided during FF (243 ± 150 ml) was significantly (P < 0.0001) lower than voided volume IF (344 ± 156 ml). PVR after FF (24 ± 59 ml) was significantly lower (P < 0.0001) than PVR after IF (70 ± 106 ml). BVE IF (82.9 ± 24.7) was significantly lower than BVE FF (92.3 ± 14.2) (P < 0.0001). Table 1 and Figure 1 compared BVE FF and BVE IF for predominant urinary incontinence complaints.
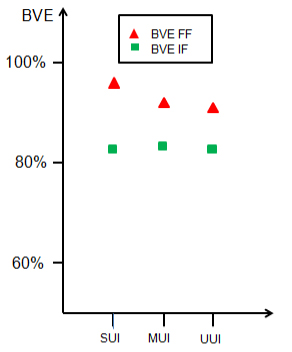
Figure 1. Variation in BVE evaluation between free uroflow (BVE FF), red triangles and intubated flow (BVE IF) green squares vs. predominant urinary incontinence complaint.
Influence of age
When factoring the role of age on BVE, the data was separated in three age categories according to menopausal status: 20–45 years old, women of reproductive age (pre-menopause), 46–65 years old (peri-menopause), and > 65 years old (post-menopause) (Table 2).
BVE IF was significantly different in women in the peri-menopause and older groups. Moreover, because PVR influences the BVE findings and a significant increase of PVR was only observed for the subgroups 46–65 and > 65 years, the latter two subgroups were grouped together. Therefore, the difference between 20–45 years and > 45 years sub-group categories was significant for PVR after IF (38 ± 72 vs. 80 ± 112 ml, P = 0.0061) while PVR after FF did not show any difference (18 ± 28 vs. 26 ± 66 ml).
Finally, when the main complaint was urinary incontinence, BVE IF was significantly lower than BVE FF in the subgroup of women aged > 45 years (Table 3).
Table 1. Evaluation of bladder voiding efficiency for all women with urinary incontinence complaint.
|
|
|
|
| N |
52 |
71 |
65 |
| BVE FF |
96.2 ± 9.5 |
91.1 ± 15.9 |
90.5 ± 15.1 |
| BVE IF |
82.4 ± 24.6 |
83.4 ± 24.3 |
83.1 ± 25.4 |
| P |
0.0006 |
0.0189 |
0.0401 |
Table 2. Influence of age on BVE value.
|
|
|
|
|
| 20–45 |
43 |
91.1 ± 17.5 |
92.1 ± 14.9 |
0.7803 |
| 46–65 |
75 |
84.5 ± 22.7 |
94.2 ± 13.1 |
0.0027 |
| > 65 |
70 |
76.3 ± 28.6 |
90.6 ± 14.9 |
0.0002 |
Table 3. Influence of age vs. predominant urinary incontinence complaint on BVE value.
|
|
|
|
|
|
| 20–45 |
|
43 |
15 |
13 |
15 |
| |
BVE FF |
|
95.5 ± 11.8 |
94.9 ± 6.2 |
86.2 ± 21.0 |
| |
BVE IF |
|
92.4 ± 14.2 |
82.8 ± 22.9 |
88.0 ± 21.9 |
| |
P |
|
NS |
NS |
NS |
| > 45 |
|
145 |
37 |
58 |
50 |
| |
BVE FF |
|
96.8 ± 7.8 |
90.9 ± 16.8 |
91.0 ± 13.7 |
| |
BVE IF |
|
77.8 ± 26.9 |
80.9 ± 25.6 |
81.9 ± 26.1 |
| |
P |
|
0.0003 |
0.0099 |
0.0265 |
DISCUSSION
Bladder voiding efficiency (BVE or void%) quantifies the voiding efficacy or percentage of bladder emptied. Easy to calculate, the bladder voiding efficiency index is seldom used. Should a clinician decide to incorporate this index in her patient care, for example in the management of urinary incontinence, one is confronted by the fact that there has been no studies published to date to establish if the bladder voiding efficiency index should be derived from a free flow or from an intubated flow.
Therefore, benefiting from a large urodynamic dataset, we decided to compare the bladder voiding efficiency index in women studied on the same day with a non-invasive flow or free flow first and then an intubated flow at the conclusion of their urodynamic session. We also were interested in examining the effect of aging on this measurement, as well as study a possible correlation between bladder voiding efficiency and presenting complaints and urodynamic findings of urinary incontinence.
Three main findings were observed. First, the free flow may be sufficient, since the catheter may provoke voiding artefacts that could affect the bladder voiding efficiency values obtained during an intubated flow study. Second, the presence of a catheter can also affect the result of the bladder voiding efficiency calculations with aging as it is harder for an older detrusor to void across a urethral catheter, no matter how small the catheter is. Finally, the bladder voiding efficiency index can be useful in the management of women with UI because this parameter is more encompassing than the post-void residual alone as it takes into consideration the initial bladder volume.
There is a relative dearth of information in the current literature on the clinical relevance of bladder voiding efficiency. Paul Abrams (BJU 1999) argued that bladder contractility (bladder contractility index) or performance during voiding (bladder voiding efficiency) should be assessed [
1]. Back then, the interest was focused on defining obstruction in men and predicting who might be benefiting from prostatic outflow-relieving procedures. In this era when a greater focus has been placed on investigating detrusor underactivity, such an index may become a useful tool again.
As defined by Dr. Abrams, bladder voiding efficiency “is a product of bladder contractility against urethral resistance and is measured according to the degree of bladder emptying”. This definition suggests that some element of urethral resistance should be present to best calculate bladder voiding efficiency, hence justifying our study looking at the effect of a urethral catheter present inside the urethral lumen during a urodynamic study in women. Likewise, because the bladder voiding efficiency index is greatly dependent on post-void residual, the post-void residual is dependent on effect of aging in this studied population. As mentioned by Dr. Abrams, this parameter may be essential when studying a group of patients on “drug trial or before/after a surgical intervention”. He was referring at the time to “lower urinary tract symptoms suggestive of benign prostatic obstruction”, but the same could apply to the medical management of women with urinary incontinence or the outcome of an anti-incontinence surgical procedure.
An argument to favor BVE calculated from a free flow rather than an intubated flow comes from the concern that a urethral catheter can impact voiding performance. Using a mathematical model, VBN, we have previously demonstrated that a 7 F urethral catheter produces no significant geometrical obstruction [
5] but can induce a urethral reflex [
6]. So, although according to Dr. Abrams’ definition cited above some element of urethral resistance is desirable to best calculate bladder voiding efficiency, in women, our data suggest that the resistance produced by a urethral catheter may induce sufficient variations in bladder voiding efficiency to prefer studying this index in a non-catheterized condition. In their study on male bladder voiding efficiency, Bosch
et al. [
7], concluded that PVR may not always be comparable to PVR measured after a free uroflowmetry in the same patient but they did not compare data from FF and IF. So the debate remains unsettled for BVE measured in men.
A great merit of bladder voiding efficiency is that this index takes into account the bladder volume at initiation of voiding and the post-void residual volume. So, it is superior to the evaluation of the PVR volume only. We observed that in women of reproductive age, bladder voiding efficiency measured from a FF is comparable with bladder voiding efficiency obtained during an IF, and this was true regardless of the presenting complaint. However, in the older subgroups (> 45 years and older) we noticed a decrease of BVE when the main complaint was urinary incontinence. So, our study outlined the role of ageing in evaluation of BVE and suggests a possible effect of detrusor dysfunction increasing over time in women. A larger sample size and longitudinal data in an observational cohort will be needed to confirm this finding.
Mostly studied in men so far [
4,
7], data on BVE in women is scarce. In one study by Cholhan
et al., premenopausal patients aged 18 to 45 underwent BVE measurements at two separate visits during their cycle, one initially during their proliferative phase and the second one during their secretory phase [
2]. The testing was done the same way at both visits, starting with a free flow first, then each subject was catheterized (catheter size not mentioned) and filled with 400 ml. The catheter was removed and a second free flow was obtained. In this relatively healthy and young population with median post-void residuals less than 50 ml, median BVE values for both studies were consistently above 90%. In their conclusion, the authors recognized the need for a future comparative study of BVE in normal and diseased subjects. Hence, our focus on women referred with complaints of urinary incontinence for urodynamic testing to elucidate the mechanism(s) of their incontinence. Even though our data was acquired differently than theirs, it confirmed their findings in a younger age group. However, we were able to explore older age groups, despite the fact that our data lacked age-matched non incontinent patients. To compensate for this lack of comparative information, we looked at other urodynamic indications in the older age categories, but our sample size was too small to allow us to draw meaningful comparisons.
Future studies should focus on the role of BVE to differentiate between specific diagnostic conditions while continuing to examine the role of detrusor aging which may influence the degree of post-void residual volume.
In conclusion, BVE index is a relatively simple index to measure. In this large cohort of non-neurogenic women studied urodynamically for urinary incontinence, BVE measured from a free flow was found generally higher than BVE obtained during an intubated flow. BVE after FF did not change with age and presenting urinary incontinence complaint whereas BVE after IF decreased in the peri-menopausal and older age groups, possibly due to some element of detrusor dysfunction.


